
All, Case Presentation
Single tooth restoration with one All-Ceramic Implant Solution in the anterior region

24
Mar
Mar













Dr. med. Dr. med. dent.
Thomas Mehnert
Specialist in Oral and Maxillofacial Surgery
1978-1983 – Studied dentistry at the University of Jena and at the Dresden Medical Academy
1983 – 1988 – Specialist dentist training at the Clinic for Oral and Maxillofacial Surgery / Aesthetics and Reconstructive Surgery, Klinikum Chemnitz GmbH in Chemnitz
1988 – Specialist in maxillofacial surgery
1988 – 1989 – Head of the maxillofacial surgery department of the polyclinic at the Chemnitz Clinic
1989 – 1992 – Senior Physician of the Department of Oral and Maxillofacial Surgery St. Lukas Klinik Solingen
1990 – 1991 – Studied medicine at the Dresden Medical Academy
1991 – Doctorate in Dr. med., University of Mainz
1992 – Specialist in oral and maxillofacial surgery
1992 – Branch in own practice with an extra bed department at the Evangelical Hospital Cologne / Kalk
1993 – Additional designation “plastic operations”
1999 – Certification focus on “implantology”
2000 – Doctorate in Dr. med. dent., University of Cologne
Since 2002 – Consultant for implantology
Memberships in scientific associations:
Two-piece ceramic implants from the latest generation (ZrO2) are trending in the dental market nowadays because of its excellent biological and material technology characteristics as the alternative treatment option compared to titanium implants [1-11]. The handling and the Workflow now correspond to the Demands of modern implantology. The successful use of two-piece Ceramic implants is presented in this clinical case.
Case presentation
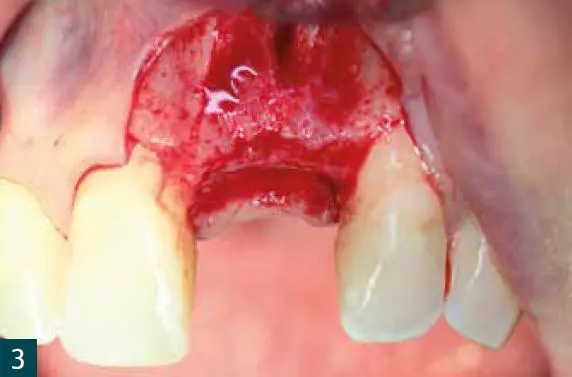
A 40-year-old patient presented with a tooth 21 that was not worth preserving in our jaw surgery practice before (Fig. 1). The tooth film shows an approx. 7 mm in size apical lightening with widening of the periodontal gap in the upper third of the root (Fig. 1). In view of the clinical situation (high smile line, good oral hygiene) decided we are looking for a two-part ceramic implant Zeramex XT (Dentalpoint AG).
Surgical phase
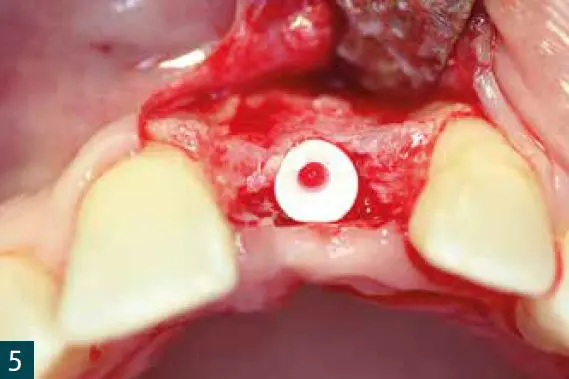
After extraction of tooth 21, the excochleation of the apical granulation tissue via a semilunar incision (Fig. 2). To avoid failure of the ossification of the ceramic implant and the soft tissue structures (papillae, to protect attached gingiva), we chose a two-stage one Action. A clampless prosthesis made of Valplast served as a temporary restoration. Region 21 was opened after five months (Fig. 3). A two-part ceramic implant Zeramex XT (ø 4.2x L 12 mm) was incorporated (Fig. 4, 5).
The guidelines of implantation in the anterior region and the Adherence to the drilling protocol of the manufacturer was observed. In addition to the transversal, the vertical insertion depth is crucial for a prosthetic success. Because of a special thermal etching process in the collar area the implant can be inserted between 1.6 and 0.6 mm supracrestally, the insertion depth depending on the Gingival height and the existing bone of the neighboring teeth oriented (Fig. 4, 5).
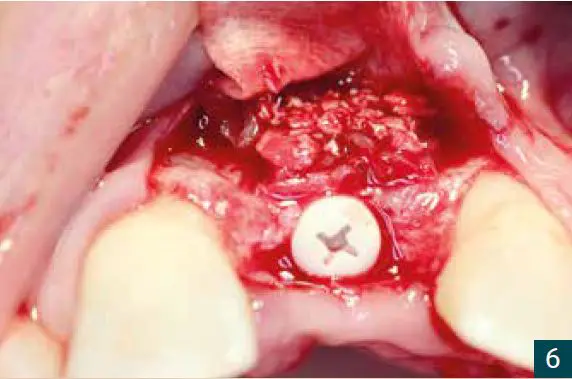
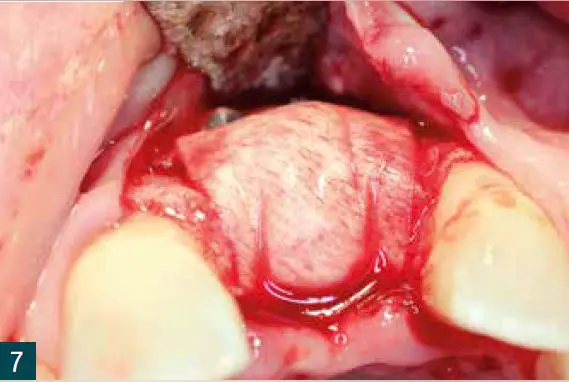
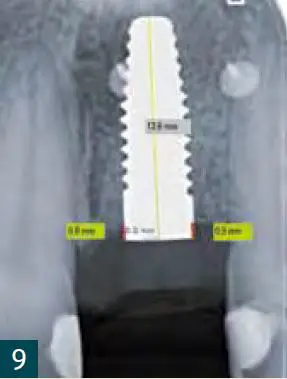
Since the abutments are applied at least one millimeter from the level of the implant shoulder, the implant should be positioned approximately two to three millimeters subgingivally. The transverse bone structure was mixed from autologous bone chips (retromolar UK), xenogeneic Bone replacement (Bio-Oss) and a membrane (Jason membrane) performed (Fig. 6, 7). After four months, the Exposure using a PEEK gingiva former (Fig. 8, 9).
Prosthetic phase
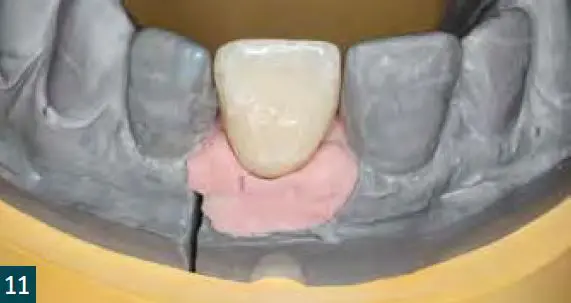
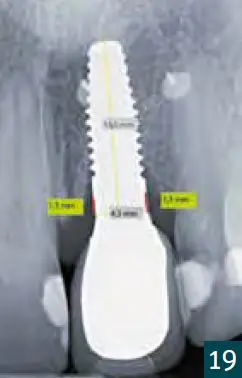
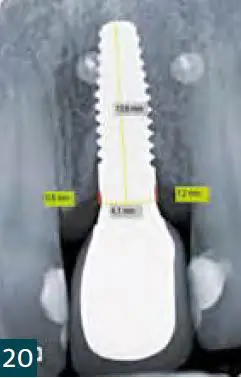
For optimal contouring of the marginal gingiva Achieving a crown in the highly aesthetic zone made from Gradia, a micro-ceramic composite. Dental film recordings (right angle technology) and the DBSWINSoftware (Dürr-Dental). There is a bone breakdown for six months (mesial bone: 0.5 mm; distal bone: 0.4 mm) and a bone structure for twelve months (mesial bone: 0 mm; distal bone: 0.3 mm) after exposure (Fig. 8, 19, 20). The yellow line on the X-ray images corresponds to the actual implant length (13.6 mm). The red lines correspond to the mesial and distal distances from the top edge of the implant to the first bone contact measured.
In our patient, the bone breakdown was in accordance with the literature in the first six months largest. However, the information in the literature in the Contrary to our supply based on one-piece ceramic implants. This phenomenon of bone cultivation is in implantology relatively rare and should be included Evidence-based long-term examinations should be backed up before one general statement. Evaluations are in progress.
Conclusion
Ceramic implants are a good addition to the titanium implants Alternative. Has the advantages of ZrO2-Ceramic itself once you get to know them, you learn to appreciate them and want to no longer do without it.
In addition to the possibility of metal-free restoration she and others For many risk groups, taking into account the indication, a useful addition to the previous treatment spectrum. He believes that the material is relatively new but somewhat different Author user training recommended. This demand for training in handling new materials will also increasingly discussed in the literature.
Dr. med. Dr. med. dent. Thomas Mehnert can be reached at:
0221 2577221 | [email protected]
Mehnert / Stember | Neumarkt 36 – 38, 50667 Cologne
ZERAMEX®XT has a tapered design allowing optimal primary stability. The internal connection has been specifically engineered to maximize the strength of rigid zirconia and eliminate any lateral forces on zirconia.
The precise fitting components offer variable placement close to bone level for enhanced restorative margin. The heart of the connection is the VICARBO® screw. Comprised of many individual threads of carbon fiber that run vertically, uncut down the length of the screw to durably absorb the tensile forces and give the VICARBO® screw its exceptionally high strength.
Learn more about this Metal-free ceramic dental implant by CLICKING HERE.
Want to know more about Zeramex?
Email us at [email protected] with your contact details and we will get in touch with you!
Click here to download the Zeramex sales brochure
Comments are closed.